How to reduce denials, ensure compliance, and optimize reimbursement for this common autoimmune thyroid disorder.
ICD-10 Coding for Graves’ Disease: The Complete Billing Guide to Autoimmune Hyperthyroidism
The Financial Impact of Graves' Disease Billing
Graves’ Disease, also known as toxic diffuse goiter, is a chronic autoimmune condition where the immune system attacks the thyroid gland, leading to overproduction of thyroid hormones.
While it affects up to 3% of the population (primarily women aged 20-40), for medical practices—especially endocrinology and primary care—it poses significant billing risks.
Imprecise coding (like using generic “Hyperthyroidism”) leads to claim denials, lower Risk Adjustment (HCC) scores, and missed revenue for expensive procedures like Radioactive Iodine (RAI). Untreated or miscoded cases can escalate to life-threatening thyroid storms, while billing errors inflate accounts receivable. Additional complications include mental health impacts (anxiety/depression), fertility issues, and sleep disturbances, all of which require precise coding for full reimbursement.
At AAA Medical Billing (AAAMB), we turn these complexities into revenue opportunities. This guide covers essential ICD-10 codes, documentation strategies, and FY 2026 updates to ensure your claims are paid clean and fast.
Official Description & Classification: The Key Codes
ICD-10 Code Range: E05.- (Thyrotoxicosis [hyperthyroidism])
Primary Billable Codes
- 00: Thyrotoxicosis with diffuse goiter without thyrotoxic crisis or storm.
- Standard code for uncomplicated Graves’ disease.
- 01: Thyrotoxicosis with diffuse goiter with thyrotoxic crisis or storm.
- Use for acute, life-threatening exacerbations (requires urgent care/ICU).
- 90: Thyrotoxicosis, unspecified.
- Bridge code pending confirmation. Avoid for recurring visits.
When to Use These Codes
Apply E05.00 as the primary code when lab evidence (elevated TSI antibodies) confirms Graves’ disease. Use E05.01 only for thyroid storm cases to justify high-level critical care billing (CPT 99291). Avoid staying on E05.90 too long, as payers may flag it for lack of specificity.
Document Synonyms: Synonyms include Graves-Basedow Disease, Exophthalmic Goiter, Hyperthyroidism due to Graves’ Disease, Parry Disease, and Basedow’s Disease document these in the notes but always code under E05.-.
FY 2026 ICD-10 Update Alert
Effective October 1, 2025, the E05 codes remain unchanged. However, CMS guidelines now stress greater specificity for autoimmune disorders. Payers are increasingly auditing “unspecified” codes.
- New Consideration: 2 (Thyroid orbitopathy) is a non-billable header code for Graves’ ophthalmopathy. You must use specifics like H06.20 (unspecified) and code also the underlying condition (e.g., E05.00).
- AAAMB Strategy: Transition patients from generic codes to specific E05.0- codes within the first two visits to prevent automated denials.

Moving Beyond Basics: Causes & Comorbidities
Graves’ Disease arises from an autoimmune response where thyroid-stimulating immunoglobulin (TSI) antibodies mimic TSH, overstimulating the thyroid.
- Genetic Factors (80%):g., HLA genes; often familial but not fully inherited.
- Environmental Triggers (20%): Stress, pregnancy/postpartum, infections/viruses, smoking (doubles risk), iodine excess, neck radiation, and certain drugs (e.g., amiodarone).
The disease rarely affects just the thyroid—to maximize reimbursement, you must code the systemic manifestations.
Cross-Reference Codes (The Revenue Multipliers)
Transition from a single-code claim to a multi-specialty claim by adding these secondary diagnoses:
- Thyroid Eye Disease (Ophthalmopathy):
- Affects up to 50% of patients; 10% severe.
- 2: Thyroid orbitopathy (Non-billable header).
- 20: Thyroid orbitopathy, unspecified.
- 20: Exophthalmos, unspecified (Bulging eyes; add laterality: .1 right, .2 left, .3 bilateral).
- Note: Code also underlying Graves’ (E05.-).
- Dermopathy (Pretibial Myxedema):
- L99: Other disorders of skin and subcutaneous tissue in diseases classified elsewhere.
- Cardiac Complications:
- 91: Unspecified atrial fibrillation (A-Fib, common in 10-15%).
- 1: Bradycardia; R00.0: Tachycardia.
- Bone Issues:
- 0: Age-related osteoporosis without current pathological fracture.
- Mental Health:
- 9: Anxiety disorder, unspecified.
- 9: Major depressive disorder, unspecified.
- Pregnancy-Related (High Risk):
- 28-: Other endocrine, nutritional and metabolic diseases complicating pregnancy. Always list O-code first, followed by E05.00.

Clinical Documentation: The Foundation for Clean Claims
Billers cannot code what doctors do not document. Vague notes lead to 20-30% denials in endocrine claims.
Key Elements to Document:
- Symptoms: Goiter size/enlargement, fine tremors, exophthalmos (bulging eyes with irritation/pressure/pain), rapid heartbeat (>100 bpm), unintentional weight loss despite increased appetite, heat intolerance, fatigue, anxiety/irritability, sleep disturbances, increased bowel movements, hair thinning, menstrual irregularities.
- Triggers/Risks: Genetic/family history, environmental (stress, smoking, infections, pregnancy), onset (gradual over weeks/months or acute).
- Lab Confirmation: Low TSH (<0.4 mIU/L), High free T3/T4, Positive TSI antibodies (>1.75 IU/L).
- Complications: Eye (double vision, light sensitivity), skin (thickened/reddened shins), cardiac (palpitations, A-Fib), bone density loss.
Why it matters: If you order a Thyroid Scan (CPT 78014), notes saying “Graves’ disease with elevated TSI, palpable nodule, and smoking history triggering symptoms” prove medical necessity, preventing the claim from being denied as “investigational.”
The Diagnostic Process & Revenue Opportunities
Diagnosis combines history, exam, and tests—all of which are billable events.
Physical Exam
Palpate thyroid for goiter; assess tremors, eye protrusion, skin changes, vitals (HR, BP).
Diagnostic Testing (High-Value Codes)
- Labs:
- CPT 84443:
- CPT 84439: Free T4.
- CPT 83520: TSI Antibody (Specific for Graves’).
- Imaging:
* **CPT 76536:** Thyroid Ultrasound (Soft tissues of head/neck).
* **CPT 78014:** Thyroid Uptake and Scan (Nuclear Medicine).
- Cardiac/Specialized:
- CPT 93000: ECG (If patient has palpitations).
- CPT 92002: Ophthalmic exam for eye disease.
- CPT 10021: Fine-needle aspiration (if nodule present).
AAAMB Tip: Check Local Coverage Determinations (LCDs) for lab frequency. If testing TSH more often than standard guidelines, document “Uncontrolled Status” or “Medication Adjustment” to justify medical necessity.

5. Billing Guidelines & Strategies to Stop Denials
Common Denial Traps
Trap 1: "Lack of Specificity"
● Issue: Using the non-billable header code E05.0 or E05.90 long-term.
● Fix: Always use the 4th/5th digit (E05.00 or E05.01); audit charts quarterly.

Trap 2: "No Medical Necessity"
● Issue: Billing for Thyroid Storm (E05.01) without supporting vitals.
● Fix: Ensure vitals (fever >101°F, HR >140) and symptoms (agitation, delirium) are in the note; appeal with labs.
Modifier Usage
- Modifier 25: Use when performing a significant E/M visit (99214) and a procedure (like Ultrasound 76536) on the same day.
- Without Modifier 25, the office visit will be bundled and unpaid, losing $50-100 per claim.
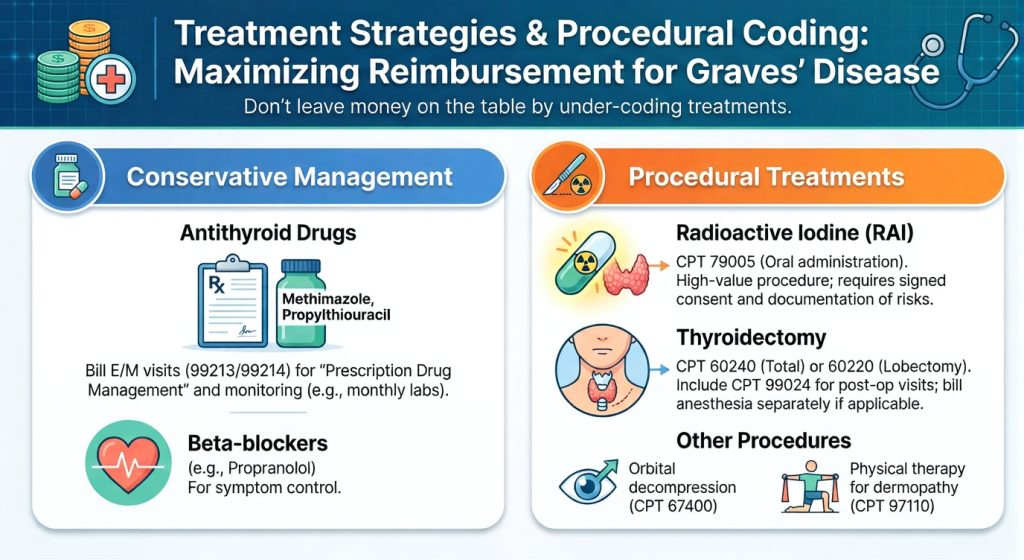
Treatment Strategies & Procedural Coding
Don’t leave money on the table by under-coding treatments.
Conservative Management
- Antithyroid Drugs (Methimazole, Propylthiouracil): Bill E/M visits (99213/99214) for “Prescription Drug Management” and monitoring (e.g., monthly labs).
- Beta-blockers (e.g., Propranolol): For symptom control.
Procedural Treatments
- Radioactive Iodine (RAI): CPT 79005 (Oral administration). High-value procedure; requires signed consent and documentation of risks.
- Thyroidectomy: CPT 60240 (Total) or 60220 (Lobectomy). Include CPT 99024 for post-op visits; bill anesthesia separately if applicable.
- Other: Orbital decompression for severe eye disease (CPT 67400); Physical therapy for dermopathy (CPT 97110).
Real World Case Studies
Case A: Uncomplicated Graves'
- Scenario: 35-year-old female with anxiety, goiter, weight loss, and positive TSI antibodies; no crisis.
- Correct Coding:
- Primary:00.
- Procedure: CPT 76536 (Ultrasound) + 84443 (TSH).
- Outcome: Full reimbursement; establishes chronic care plan for ongoing monitoring.
Case B: Graves' with Eye Disease & Storm
- Scenario: 50-year-old with heart rate 150 bpm, fever, severe exophthalmos, and agitation; ER admission confirms storm.
- Correct Coding:
- Primary:01 (Thyrotoxic crisis).
- Secondary:20 (Thyroid orbitopathy, unspecified).
- Procedure: CPT 93000 (ECG) + 79005 (RAI referral post-stabilization).
- Outcome: High-level E/M paid due to crisis code; secondary code justifies eye care referral and avoids denial.
Case C: Pregnancy-Complicated Graves'
- Scenario: 28-year-old pregnant woman with hyperthyroidism, goiter, and mild eye bulging in second trimester.
- Correct Coding:
- Primary:280 (Endocrine disorder complicating pregnancy).
- Secondary:00 + H05.20 (Exophthalmos).
- Procedure: CPT 84443 (TSH) + 76536 (Ultrasound).
- Outcome: Maternity billing approved; prevents complications like preterm birth.
What Our Clients Say
Our clients trust us to deliver exceptional service that makes a real difference in their practice. Here’s what some of them have to say:
Reviews
We are so grateful to AAA Medical Billing and for their incredible support of the Orland Trojan Basketball program!
Because of generous sponsors like AAA Medical Billing, we’re able to have amazing opportunities for these young boys & girls.
- Orland Trojan Basketball
- Emily N.
- Keith

Clinical Guidelines & FAQs
- Guidelines: Per American Thyroid Association (ATA): Start with antithyroid drugs for 12-18 months; opt for RAI or surgery if remission fails. Monitor TSH/T4 every 4-6 weeks initially, then quarterly. For eye disease, involve ophthalmology early. Avoid iodine contrast in imaging for at-risk patients.
Final Words: Safeguard Your Revenue with Expert Support
Graves’ Disease demands precise coding to navigate its autoimmune complexities and comorbidities. With accurate E05 use, robust documentation, and denial-proof strategies, you can achieve 99% clean claims and under 1% rejections.
At AAAMB, our global team of 550+ experts handles 30+ specialties with 24/7 support. Losing money on thyroid claims? Contact us for a free audit—convert denials to revenue starting at just 2.95%.