How to reduce denials, ensure compliance, and optimize reimbursement for one of the most common and complex medical complaints.
Mastering ICD-10 Code R42: The Revenue Cycle Guide to Billing Dizziness & Giddiness
The High Cost of Dizziness
In the fast-paced world of healthcare, dizziness is a ubiquitous complaint. Whether it’s a senior citizen fearing a fall or a young professional experiencing sudden vertigo, patients seek answers.
However, for medical practices, dizziness presents a silent financial threat. Relying too heavily on the generic ICD-10 code R42 without proper documentation is a leading cause of claim denials for diagnostic testing (like MRIs) and specialized procedures.
At AAA Medical Billing (AAAMB), we believe precise coding is the bridge between clinical care and financial health. This guide breaks down everything you need to know about R42 from clinical definitions to FY 2026 coding updates—to keep your revenue cycle stable.
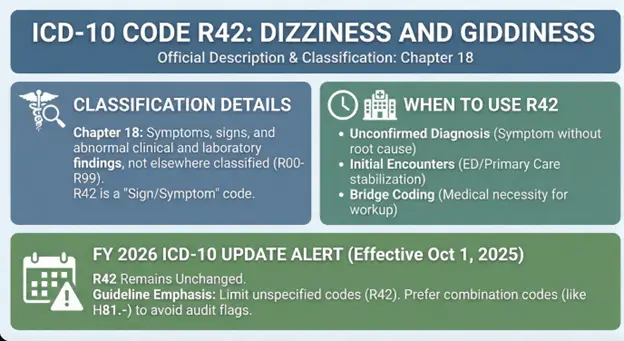
Official Description & Classification: What is R42?
ICD-10 Code: R42
Dizziness and giddiness
Chapter 18: Symptoms, signs, and abnormal clinical and laboratory findings, not elsewhere classified (R00-R99).
When to Use R42
R42 is a “Sign/Symptom” code. It is designed for use when:
The diagnosis is unconfirmed: The patient has symptoms, but tests haven’t yet revealed the root cause.
Initial Encounters: Common in Emergency Departments (ED) or primary care visits where immediate stabilization is the goal.
Bridge Coding: It establishes medical necessity for the diagnostic workup required to find a diagnosis.
FY 2026 ICD-10 Update Alert
As of FY 2026 (effective Oct 1, 2025), R42 remains unchanged. However, general guidelines continue to emphasize proper use of symptom codes: Unspecified codes like R42 should only be used when documentation lacks detail for specificity. Payers scrutinize them for recurring visits. Using R42 as a primary diagnosis without progressing to a more specific code (like H81.-) may trigger automated audit flags. Combination codes are preferred where applicable to fully identify conditions.
2. Moving Beyond R42: Causes & Cross-Reference Codes
To maximize reimbursement, providers must transition from the generic R42 to specific disease codes as soon as a diagnosis is confirmed.
A. Inner Ear Disorders (The Most Common Transition)
If testing confirms a vestibular issue, stop using R42 and use the H-Series: BPPV (Benign Paroxysmal Positional Vertigo): Use H81.1- (Requires laterality: Right, Left, or Bilateral). Ménière’s Disease: Use H81.0-. Labyrinthitis: Use H83.0.
B. Cardiovascular Issues
Orthostatic Hypotension: Use I95.1 (Often requires tilt-table testing results). Arrhythmias: Use I49.-.
C. Neurological Conditions
Vestibular Migraines: Use G43.x. Stroke/TIA: Use I63.- (Stroke) or G45.x (TIA). Note: These are high-acuity codes that justify emergency level E/M billing.
D. Psychological Factors
Psychogenic Dizziness: Use F45.8. Anxiety Disorders: Use F41.0 (Panic disorder).

Clinical Documentation: The Key to Clean Claims
Billers cannot code what doctors do not document. To ensure R42 (and subsequent testing) gets paid, clinical notes must be specific.
Key Descriptors to Document:
Type: “Spinning” (Vertigo) vs. “Lightheaded” (Presyncope) vs. “Unsteady” (Disequilibrium).
Triggers: “Worse when rolling over in bed” (Suggests BPPV) vs. “Worse upon standing” (Suggests Orthostatic Hypotension).
Associated Symptoms: Nausea, tinnitus, hearing loss, or headaches.
Why this matters: If a provider orders a Brain MRI (CPT 70551) for “Dizziness, insurance may deny it as investigational. However, documenting “Dizziness accompanied by focal weakness and slurred speech” justifies the MRI under medical necessity guidelines.
The Diagnostic Process & Revenue Opportunities
Proper evaluation of dizziness is thorough and billable.
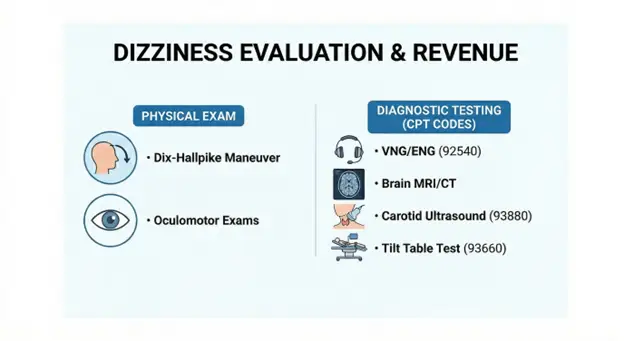
Physical Exam
Dix-Hallpike Maneuver: Used to diagnose BPPV.
Oculomotor Exams: Checking for nystagmus (involuntary eye movement).
Diagnostic Testing (High-Value Codes)
VNG/ENG (Videonystagmography): CPT 92540. The gold standard for testing inner ear function.
Brain MRI/CT: To rule out stroke or tumors.
Carotid Ultrasound: CPT 93880.
Tilt Table Test: CPT 93660.
AAAMB Tip: Ensure your billing team checks for Local Coverage Determinations (LCDs). Some payers require a documented trial of medication (like Meclizine) before approving advanced VNG testing.
Billing Guidelines & Strategies to Stop Denials
This is where the money is made or lost.
Common Denial Traps
Trap 1: "Not Medically Necessary"
Cause: Using R42 alone for high-cost imaging. Strategy: Add secondary diagnosis codes (e.g., Z91.81 - History of falling) to strengthen the case.

Trap 2: Unspecified Code Limits
Cause: Some payers reject R42 after the 2nd or 3rd visit. Strategy: AAAMB auditors flag charts where R42 is used repeatedly. We query the provider to see if a more specific diagnosis has been found.
Modifier 25 Usage
If a patient comes in for dizziness and receives a significant, separately identifiable evaluation plus a procedure (like an Epley Maneuver) on the same day:
Bill the E/M code (e.g., 99213) with Modifier 25.
Bill the procedure code (e.g., 95992) separately.
Without Modifier 25, the office visit will be bundled into the procedure, causing revenue loss.

Treatment Strategies & Procedural Coding
Don’t leave money on the table by only billing for the “visit.”
Canalith Repositioning (Epley Maneuver)
CPT Code: 95992.
Gap Fill: Many general practitioners perform this maneuver but only bill an office visit. This is a distinct procedural service that reimburses at a higher rate.
Vestibular Rehabilitation Therapy (VRT)
CPT Code: 97112 (Neuromuscular re-education).
Usage: For long-term management of chronic dizziness.
Real-World Case Studies
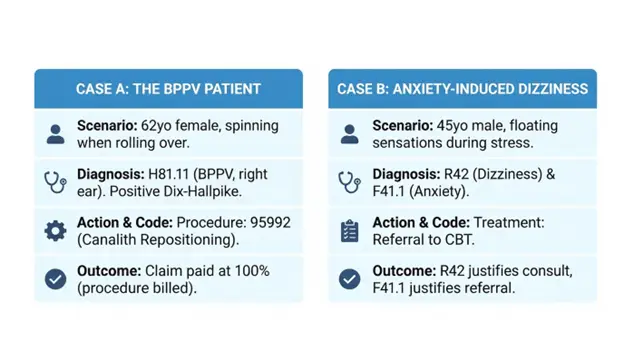
Case A: The BPPV Patient
Scenario: A 62-year-old female presents with spinning dizziness when rolling over.
Diagnosis: Positive Dix-Hallpike test confirms BPPV.
Correct Coding:
Primary: H81.11 (Benign paroxysmal vertigo, right ear).
Procedure: 95992 (Canalith repositioning).
Outcome: Claim paid at 100% of allowable rate.
Case B: The Anxiety-Induced Dizziness
Scenario: A 45 year old male reports floating sensations during work stress. No vestibular findings.
Diagnosis: Psychogenic dizziness.
Correct Coding:
Primary: R42 (Dizziness and giddiness) – Initial visit.
Secondary: F41.1 (Generalized anxiety disorder).
Treatment: Referral to CBT.
Outcome: R42 allows for the medical rule-out, while F41.1 justifies the counseling referral.
What Our Clients Say
Our clients trust us to deliver exceptional service that makes a real difference in their practice. Here’s what some of them have to say:
Reviews
We are so grateful to AAA Medical Billing and for their incredible support of the Orland Trojan Basketball program!
Because of generous sponsors like AAA Medical Billing, we’re able to have amazing opportunities for these young boys & girls.
- Orland Trojan Basketball
- Emily N.
- Keith

Final Words: Protect Your Practice with Expert Billing
Dizziness is clinically complex, but your billing doesn’t have to be. Accurate use of R42, timely transition to specific H-codes, and capturing procedural revenue (like CPT 95992) are essential for a healthy bottom line.
At AAAMB, we specialize in identifying these revenue gaps. Our team ensures that your documentation supports your claims, reducing denials and accelerating cash flow.
Is your practice losing money on "unspecified" codes?
Contact AAAMB today for a free audit of your recent R42 claims. Let us turn your dizziness denials into paid revenue.